Case Study — Fourteen Years Of Recurring Low Back Pain
9 min read
Align Pain & Performance · Clinical case study · The client, Jesse Eberle.
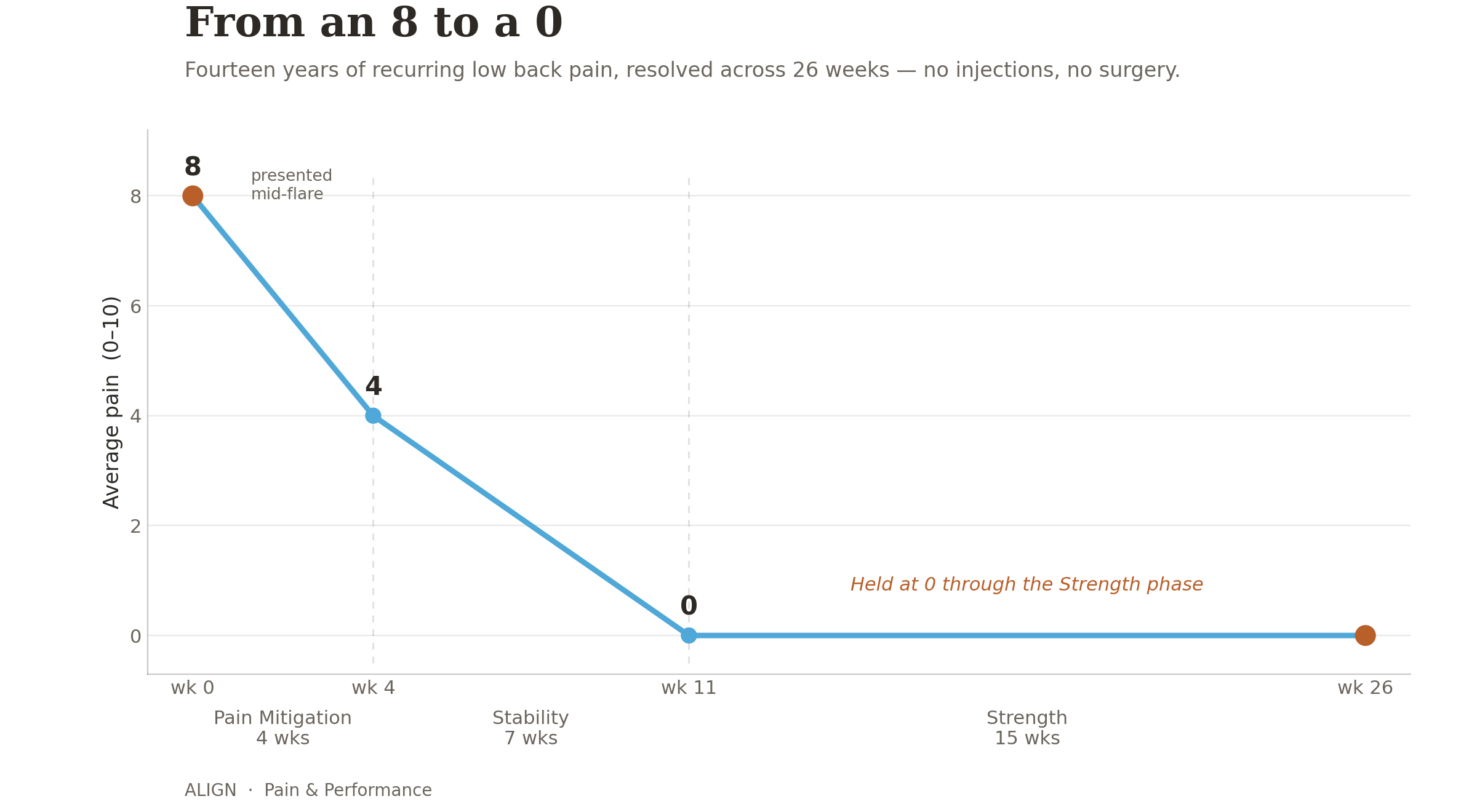
Outcome in one line: A 44-year-old man had lived with low back pain for 14 years — a constant reported pain level of 3–4 out of 10, with punishing flares to an 8 out of 10 that forced him to choose between playing with his kids and days of suffering. Across a 26-week course of mobility, stability, and strength work — no injections, no surgery — his pain resolved to 0 out of 10, the flares stopped, and he returned to hiking, biking, yard work, and his kids without paying for it afterward.

Snapshot
Client: Jesse Eberle, 44
Duration: 14 years — began with a dirt-bike crash, progressively worse over time
Location: Central low back, right-dominant
Baseline pain: Constant 3–4 out of 10, with ~6 flares a year spiking to 8 out of 10 for weeks at a time
Prior care: Anti-inflammatories, chiropractic, massage, stretching, general exercise; MRI and surgical consult ruled out any structural cause
Pain type (our determination): Chronic, primary mechanical (nociceptive); minimal nervous-system contribution
Outcome: Pain 8 → 0 out of 10; flares eliminated; full return to an active lifestyle
Course: ~26 weeks — Pain Mitigation (4 wks) → Stability (7 wks) → Strength (15 wks)
Presentation
Jesse had lived with low back pain for 14 years. It began with a dirt-bike crash and had worsened ever since — a constant ache of 3–4, punctuated by roughly six major flares a year that climbed to an 8 and lasted for weeks. Over time the flares grew more frequent, more painful, and more limiting. The pain sat centrally in the low back, more on the right, presenting as a constant ache of 3–4 out of 10 with spasms during the big flares that reached 8 out of 10.
The flares were almost always triggered by ordinary life under load: playing with his kids, yard work, working on houses, bending or lifting, or travel. Long periods on his feet left the area fatigued. What relieved it was lying down, rest, and reducing mechanical load — the classic signature of load-driven pain.
The cost was measured in impossible choices. He had to decide whether to play with his kids and then suffer for three days, or not play with them at all. He had to choose between doing his job and enduring two weeks of excruciating pain. He could no longer go on bike rides, hikes, or long walks, or work in his yard. What he wanted back was simple and important: his active life — hiking, biking, long walks, working in the yard, working on houses, and playing with his young kids.
By the time he reached us he had already tried anti-inflammatories, chiropractic, massage, stretching, and general working out. An MRI and a surgical consult had excluded any structural cause for the pain.
The Reasoning: A Process of Exclusion
We do not begin by guessing a cause. Persistent low back pain spans roughly 60 contributing variables across three systems — mechanical, immune/inflammatory, and nervous system — cutting across as many as 18 medical specialties. No single diagnosis explains it, and no single specialty owns it. The work is to identify the pain type from presentation, then systematically exclude and resolve probable drivers until the pain is gone.
Step 1 — Acute vs. chronic
This was unmistakably chronic. The original injury — a crash 14 years earlier — had healed long ago; the tissue that was damaged in that crash was not the source of pain a decade and a half later. Acute pain resolves with healing. His did not, which places the entire problem in a different framework and rules out treating it like a fresh injury.
Step 2 — Pain-type identification
His pain was clearly primary mechanical (nociceptive), with very little nervous-system driver. The evidence:
Mechanical load made it worse; reducing load made it better. Bending, lifting, play, yard work, and time on his feet drove flares; lying down and rest relieved it.
Stress and sleep fluctuations did not track with his pain. A nervous-system-dominant pain would flare with poor sleep or stress; his did not.
He carried none of the psychosocial risk factors for nervous-system pain — high sleep quality, low stress, strong social connection, low anxiety, no widespread pain.
The only nervous-system amplifier present was the sheer duration — 14 years of pain can create some peripheral and central sensitization. Worth noting, but not the lever.
Step 3 — Narrowing the field
Those ~60 possible drivers are spread across all three systems. Because his pain was clearly mechanical, his real drivers concentrate in the mechanical share of that list, and the immune and nervous-system contributors drop down the priority order. His MRI and surgical consult had already excluded structural causes. With structure off the table, the mechanical field reduces to three categories:
Mobility — joint range of motion.
Stability — joint position and neuromuscular balance (how load gets distributed).
Strength — the load-bearing capacity of the joint system and tissues.
Assessment Findings
The evaluation found dozens of discrete mechanical drivers.
Mobility — his measured range, with the functional norm for comparison
Hip external rotation: 45° (normal is ~90°) — half of normal.
Hip internal rotation: 20° (normal is ~40°) — half of normal.
Hip extension: 3° (normal is 10–15°) — the leg could barely move behind the body.
Hip flexion: 30° (normal is 65–90°) — less than half; measured as a straight-leg raise, it reflects how tight his hamstrings were.
Spine rotation: 40° (normal is ~90°) — less than half the available rotation.
Ankle dorsiflexion: 35° (normal is 45–60°) — restricted.
Stability / alignment
A severely rotated pelvis: a 2" right-sided hike, the right hip rotated 5° posterior and the left hip 10° anterior.
An obvious loss of the SI joint's force-closure mechanism during hinging — he reported a "biting," "jabbing" pain whenever he bent over.
Neuromuscular pattern
Under-active (not doing their job): glute medius/minimus, glute max, psoas, deep core (diaphragm, TVA, pelvic floor), adductors, and multifidus.
Over-driven (compensating and overloaded): TFLs, IT bands, rectus femoris, QL/lumbar erectors, piriformis, and hamstrings.
The picture: some muscles had become under-active, others were carrying loads they were never meant to, and the pelvis and spine were being asked to move through positions they could no longer control. Fourteen years of that is more than enough to keep a back in pain — with no structural damage required.
Why this is good news. None of these drivers is a life sentence; every one is correctable. Range can be restored, a pelvis can be re-aligned, under-active muscles can be re-trained, and capacity can be rebuilt. The task was simply to work through them in the right order — rebuilding enough capacity that the demands of his everyday life no longer outstripped what his back could handle.
The Intervention
Phase 1 — Pain Mitigation (4 weeks)
Goal: restore joint range of motion, reduce compensatory muscle drive and guarding, and eliminate the pelvic rotation.
He arrived mid-flare — bent sideways, pain at an 8 out of 10. We started with soft-tissue deactivations on heat with long-exhale breathing, and light rolling of the TFLs, quads, lumbar erectors, and inner thighs to calm the guarding. As things settled, we layered in static and active stretching plus eccentric loading to restore range of motion, and used seated block and belt work and cats-and-dogs to unwind the pelvic rotation.
Result: range of motion restored, pelvic alignment restored, and pain down from 8 to 4 out of 10.
Phase 2 — Stability (7 weeks)
Goal: restore neuromuscular capacity to the under-active muscles — glute medius/minimus, glute max, adductors, psoas, deep core, and lats — and re-establish the SI joint's force closure.
We built progressive strength through wall-supported clamshells, outer thigh raises, front leg raises, inner thigh raises, hip bridges, deep-core activations, and straight-arm pulldowns — retraining these under-active muscles to carry their share of the load again, so it stopped falling on the overworked compensators.
This is also how we restored the force-closure mechanism of the SI joint — the self-bracing that had failed whenever he hinged. Force closure is produced by the muscular "slings" that cross and compress the joint, so we rebuilt stability through all three: the posterior sling (glute max working with the opposite lat), the anterior sling (deep core and adductors), and the lateral sling (glute medius/minimus and adductors controlling side-to-side stability). As those slings regained strength and coordination, the joint regained its stability and the "biting, jabbing" pain on bending resolved.
Result: pain from 4 to 0 out of 10.
Phase 3 — Strength (15 weeks)
Goal: build load-bearing capacity through movements that map directly onto his life.
With pain gone, the job was to make sure it stayed gone by building capacity well above the demands of his lifestyle: squats, deadlifts (picking things off the floor), step-ups (hiking and biking), and spine stability through planks, anti-rotation, and back extensions. Load was added progressively with adequate recovery.
Benchmarks built: a 185 lb deadlift and squat, 100 lb step-ups, 5-minute planks, 40 lb anti-rotations, and 40+ reverse back extensions.
Outcome
Baseline: constant 3–4 out of 10, flares to 8 out of 10 (presented at 8 out of 10)
End of Pain Mitigation (4 weeks): 4 out of 10
End of Stability (+7 weeks): 0 out of 10
End of Strength (+15 weeks): 0 out of 10, flares eliminated
That new capacity changed the terms of his life. He no longer has to choose between playing with his kids and suffering for it. He can hike, mountain bike, work in the yard, do construction, and travel — and not hurt afterward. Total course: ~26 weeks, with no injections, no surgery, and no structural intervention.
What This Case Teaches
1. An old injury is not a life sentence. The crash was 14 years ago; that tissue healed long ago. The pain that remained wasn't the injury — it was a body that had drifted into poor mechanics and lost capacity. Chronic pain from an old trauma is no longer the trauma. It's the state of the system now — and the state of a system can be changed.
2. Flares are capacity being exceeded, not damage being done. His flares came from play, lifting, yard work — from living. The activities weren't the problem; the problem was that his capacity had shrunk below the demands of his life, so ordinary load kept tipping him over. Raise the capacity and the flares stop.
3. Avoidance is a shrinking cage. Choosing not to play with his kids to dodge pain fixes nothing — it just narrows the life while capacity keeps falling. The answer is never to do less. It's to build the capacity to do more without paying for it.
4. Persistent pain is resolved by sequence, not by diagnosis. There was no single "cause" to find — there were dozens of mechanical drivers: lost range, a rotated pelvis, under-active muscles, others overloaded. We didn't diagnose the cause; we worked the process — restore range, re-align, then rebuild stability, then load — ruling out and resolving drivers in order until the pain was gone and his strength exceeded the demands of his life.